
Behind the Study is a series of transcribed videos from researchers elaborating on their recent oncology-focused studies published in Aging. A new Behind the Study is released each Monday. Visit the Aging YouTube channel for more insights from outstanding authors.
—
Aging Editorial Board member Dr. Alex Zhavoronkov discusses his 2020 research paper published by Aging, entitled, “Geroprotective and senoremediative strategies to reduce the comorbidity, infection rates, severity, and lethality in gerophilic and gerolavic infections.”
Hello, my name is Alex Zhavoronkov and I’m the Founder and CEO of a company called Insilico Medicine. We are focused on the latest applications of artificial intelligence to drug discovery, biomarker development, and aging research. And I’m also a Chief Scientist at the Biogerontology Research Foundation. It’s a UK-based charity, 12 years old now founded in 2008. It’s called the Biogerontology Research Foundation because it’s focused primarily on biological and biomedical gerontology with support research worldwide. And we also conduct policy outreach, policy documents, and promote aging research worldwide.
We got into the coronavirus theme in mid-January as a company and also as an extended group of collaborators. At Insilico, we decided to go directly after viral proteins. So we have the ability at Insilico to identify new targets, but also to generate normal compounds very quickly using generative cell networks and reinforcement learning. So it’s kind of imaginative and strategy oriented AI to create molecules that specifically bind to the proteins of interest.
So we originally published and put out the paper and the molecules for the 3C-like main protease of the SARS-CoV-2. And we’re working with multiple collaborators worldwide to provide the molecules for their proteins of interest, and also we are generating a bunch of others. However, for the purposes of this paper we are not using AI in any way. It’s human intelligence and it is quite obvious that SARS-CoV-2 is more harmful to the elderly, the people over 50. So it’s infecting more people over 50, it is a much more severe and much more lethal in that age group.
So that is why it’s actually pretty unique compared to other viruses. So if you look at influenza and the other common viruses we do not see another virus, we do not see such effects in the elderly, so it’s a little bit more equal opportunity infections. For SARS-CoV-2 it infects mostly the elderly and there is actually no term to describe it right now. So in the paper that I put forward in Aging, I propose a new term so it’s gerophilic and gerolavic infection from Greek géros, old man and epivlavís, harmful. So it’s more harmful to the elderly, more severe in elderly. And gerophilic it’s géros again old man and philia is love, so it loves old people.
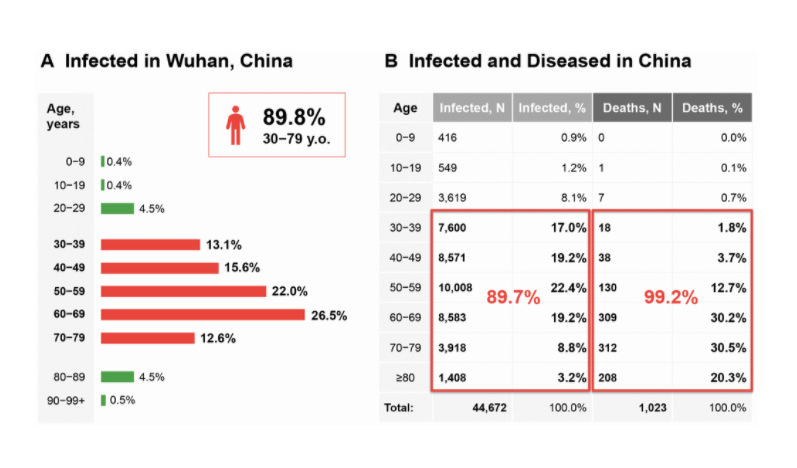
And if we’ll look at the data from Wuhan in China, you will see that 90% of the population, 89.7% of the population, who got the virus were over 30. And 99.2% of the population that died of it were over 30. So it’s really uneven distribution for both severe cases and lethal cases in the population. And one of the really important case studies that has been studied quite extensively is the Diamond Princess cruise ship. So the world’s most watched lab that came into attention because a few thousand people got stuck, very diverse population group was stuck on one cruise boat. And out of those few thousand, around 700 contracted the virus and most of them were over 65 and there were originally seven deaths, and a few more people died.
And we see that people who had the infection, even with mild symptoms, they have dark spots in their lungs on CT. So it looks like they have some lesions and there is some fibrosis. Even if the disease has mild symptoms, in the elderly more so, it leaves the fibrotic trace. And in the paper, I’m hypothesizing that the disease is associated with immunosenescence. So both the involution of the thymus and many other processes that lead to immunosenescence. Immunosenescence leads to infection, so here you have of course chances of death. Infection leads to more damage and loss of homeostasis and that leads to accelerated aging. And also acceleration of age-related pathology also increase the chances of death that lead to more immunosenescence. So it’s kind of the vicious circle of immunosenescence and infection.
And there have been many studies in the past showing that some of the geroprotectors like sirolimus, rapamycin, are maybe effective in potentiating response to vaccines and also preventing infection in the elderly. So it’s paradoxical observation that immunosuppressant, like rapamycin, might have immunostimulatory effects. And there was anecdotal evidence showing that it protects the elderly from influenza and other virus not infections. It’s pretty obvious to try something like rapamycin that is reasonably safe in low doses. So in high doses it has substantial side effects, but in low doses it’s very well tolerated.
So there are others what is called rapalogs, very famous one is called everolimus. It’s so very close structural analog to sirolimus, developed by Novartis which has claimed to be selective to specific coattails and outdoor complex that make it more beneficial for aging and for other diseases. However, I would really like to see more evidence of that because those are very close structural analogs and there are other inhibitors that serve the same purpose. So 2013, Novartis conducted few experiments with everolimus, the drug is called RAD001 and demonstrated that in healthy elderly patients a low dose treatment with RAD001. Results in even potentiation and less infection with influenza and also potentiation of vaccines. So that was promising news.
So they published in 2014 in Science Translational Medicine and it was very promising study. Then in 2018, they showed that a combination of everolimus and another ToR inhibitor also results in immune potentiation and prevention of several infections, primarily influenza. So for influenza, they published in Science Translational Medicine, and a spinoff out of Novartis took those molecules into clinic, into Phase 3. And in Phase 3, they decided to instead of using everolimus, they used the molecule called BEZ235 rebranded as RTB101 which had high concentrations. It’s also a PI-3K inhibitor, so it’s not a very selective inhibitor or ToR, and they failed in Phase 3.
But they haven’t used RAD001 or sirolimus in combination or as control. I believe that it’s likely to be because of the molecule and also patient selection, so it should be biomarker used for that. But those promising early experiments clinical studies with RAD001 and also substantial evidence from the clinic met-studies showing that rapamycin is potentiating a vaccine response and immune status in the elderly. That gives us very promising data to try sirolimus in Phase 3 in low doses maybe once a week, maybe in combination with other geroprotectors like metformin, like NAD boosters, like senolytic to potentiate the immune system of the elderly before they get sick.
So in this paper, I also want to highlight that it’s not a medical advice, it’s not a recommendation, it’s a call for a clinical trials of an alternative view on how to address COVID-19 also SARS-CoV-2 and prevent infection and increase survival in the elderly, and also make it less severe for the elderly. So in this paper, I’m calling for clinical trials of rapamycin, a very well known geroprotector. It was actually implicated in Aging by Professor Mikhail Blagosklonny at the Roswell Park Comprehensive Cancer Center in early 2000s. So 2004, 2005, 2006 with seminal papers showing that cancer agent is very likely to be also an anti-aging compound, and I now believe that this compound should be tried in multiple age associated pathologies and also for immmunosenescence, versing immunosenescence.
But other geroprotectors, promising geroprotectors, like metformin, can be very well combined with rapamycin, NAD boosters like nicotinamide riboside, nicotinamide mononucleotide may be tried in clinical trials. Senolytic, these could be tried also after COVID because of the fibrotic build-up, fibrosis in the lungs and also as rehabilitation after COVID. I think that some other promising geroprotectors including [inaudible] B3 activation. Again, that’s much less explored, could lead to gene clocks. So since 2013 there has been a revolution in gene clocks starting from our Panam and Horvath work showing that methylation data is very predictive of chronological age.
There are very highly accurate markers of aging but there are many others, so like lab tests, very simple clinical blood tests can be used to predict chronological age and my group published the first ones using deep learning. And there are many others including microbiomics aging clock, including imaging aging clocks, including transcriptomic aging clocks, and proteomics aging clocks, and whatever data there is longitudinal data that could be used to construct clocks should be collected during the clinical trials. And we should look at whether some of the molecules are making you younger or older compared to the chronological age from the various data types and look at the effects.
So that’s the current proposal on the paper, so I’m calling to try geroprotectors to protect the elderly, to potentiate their immune response to COVID, and also to try the aging clocks for both clinical trials enrollment and for monitoring to see what molecules are making you younger or older on pretty much every level. I’m also calling for those clinical trials because after COVID-19, after the epidemic is over, we’re going to have major economic consequences. There’s a lot of people who have been out of work, there’s been substantial capital influx from pretty much every government into the economy, so quantitative easing that might lead to inflation. We don’t know what’s going to happen to the economies of developed countries.
Previously, I published several papers and a book on economics of aging showing that increases in productive longevity would lead to substantial economic growth. If we manage to reduce the amount of money being spent on healthcare in the elderly by preventing disease and by rejuvenating the elderly, making them more resilient to disease, just that leads to unprecedented economic growth. And of course, if we make them more productive and contributing to the labor force longer, we will see unprecedented economic growth even further.
So we’re talking about double digit growth in developed countries. So here we can kill many birds with one stone, so to speak, even though I don’t like the word “kill.” And if we can try geroprotectors to prevent disease, but at the same time we can boost the economy after the epidemic is over if some of those geroprotectors show efficacy and people start believing more that aging is plastic and we can push the envelope in that area and really rejuvenate the elderly.
So that’s the paper and thank you very much for watching this. Stay healthy.
Click here to read the full study published in Aging.
—
Aging is an open-access journal that publishes research papers monthly in all fields of aging research and other topics. These papers are available to read at no cost to readers on Aging-us.com. Open-access journals offer information that has the potential to benefit our societies from the inside out and may be shared with friends, neighbors, colleagues, and other researchers, far and wide.

For media inquiries, please contact [email protected].